


Introduction
Individuals with sickle cell disease (SCD) experience recurrent acute vaso-occlusive events (VOE) beginning in infancy, that can be prevented with hydroxyurea therapy (Wang W. Lancet 2011), while chronic organ dysfunction becomes evident in adolescence and progresses with age. Nutritional insufficiencies and deficiencies occur in SCD (e.g., zinc, vitamin D and B6), and are associated with greater frequency of VOE (McCaskill M. Nutrients 2018, Martyres D. PBC 2016, Schall J. J Pediatr 2004). While infants and young children (age <6) are particularly vulnerable to the effects of malnutrition (e.g., developmental delay and cognitive impairment), the environmental components leading to decreased food access have not been investigated relative to the impact on their healthcare outcomes. We tested the hypothesis that restricted access to healthy food sources is associated with increased SCD-related acute care utilization among children with SCD younger than age 6 years, despite treatment with hydroxyurea.
Methods
Participants were recruited from the IRB-approved longitudinal clinical cohort study, Sickle Cell Clinical Research and Intervention Program (Hankins J. PBC 2018). Home addresses were mapped to census-tract environmental data from the US Food Access Research Atlas (USDA ERS 2017). Food deserts were defined as "low income census tracts where at least 33% (minimum of 500 people/tract) of the population live >1.0 (urban area) or >10 (rural area) miles from a grocery store or a supermarket" (Food Access, USDA ERS 2019). Three main outcomes: emergency department (ED) visits, hospitalizations, and acute care utilization (ACU=ED + hospitalizations) from a VOE, were collected from birth to age 6 and analyzed as cross-sectional outcomes at age 6-years. Generalized linear models (GLM) were used to associate environmental factors as continuous and categorical variables with the outcomes adjusted for sickle genotype and hydroxyurea exposure. False discovery rate (FDR)-adjusted p-values (pFDR) were calculated to account for multiple comparisons. Environmental factors with pFDR<0.1 were assessed in multivariate GLM. The area under ROC curves (AUC) were generated to estimate how environmental data can improve the accuracy of predicting the acute care utilization outcomes.
Results
523 children with SCD, all African American, were included. The median age at last follow-up was 5.5 years (range 1- 6), 51.7% were girls (Table 1). Differences in health care utilization and hydroxyurea use were observed according to SCD genotype. A total of 33.5 % of the studied population resided in census tracts considered food deserts. The average distance to the nearest supermarket from participants' household was 2.8 miles. Except for % of children per census tract, there were no neighborhood differences by SCD genotype (Table 1). Participant neighborhoods had on average 14.7% unemployment rate, while 30.8% of individuals were under the federal poverty threshold and received Food and Nutrition Services. 7.9% of adults had a bachelors' degree. Among the tracts where the population was considered low income, 9%
did not own a car, and the proportion of those living >0.5 and >1.0 miles from a supermarket was 37% and 16%, respectively.
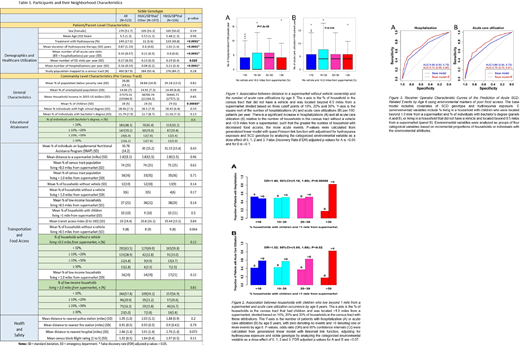
Living in a household without a vehicle and located >0.5 miles from a supermarket was associated with increased hospitalizations and ACU (Figure 1). The odds ratio (OR) of experiencing >0 hospitalizations or ACU were 1.3 (95%CI: 1.0-1.8) or 1.5 (95%CI: 1.1-2.0), for those living in a household without a vehicle and >0.5 miles from a supermarket, respectively. Living in a household with children and >1.0 mile from a supermarket was associated with high risk of experiencing >0 hospitalizations (OR: 1.5; 95%CI: 1.2-1.8) and >0 ACU (OR: 1.3; 95%CI: 1.1-1.7) (Figure 2). The accuracy of predicting a SCD-related acute event by age 6 years significantly improved when adding markers of poor food access to the predictive model (AUC increase: ≥0.06, p=0.01) (Figure 3).
Conclusion Living in food deserts limits access to affordable and nutritious foods. Food deserts are associated with poor health outcomes among pre-school children with SCD. The prediction of acute care utilization in young childhood increases when food access is considered. Treatment with hydroxyurea did not mitigate the effects of reduced food access on the frequency of acute care utilization of young children with SCD.
Estepp:ASH, NHLBI: Research Funding; Daiichi Sankyo, Esperion, Global Blood Therapeutics: Consultancy; Global Blood Therapeutics, Forma Therapeutics, Pfizer, Eli Lilly and Co: Research Funding. Hankins:LINKS Incorporate Foundation: Research Funding; National Heart, Lung, and Blood Institute: Honoraria, Research Funding; Novartis: Research Funding; UptoDate: Consultancy; MJH Life Sciences: Consultancy, Patents & Royalties; Global Blood Therapeutics: Consultancy, Research Funding; American Society of Pediatric Hematology/Oncology: Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal